We’ve heard that the “mental illness epidemic” is a major public health crisis in the US, perhaps even globally. The claim is that rates of mental illness have skyrocketed in recent decades, and now as many as 1 in 4 people have a mental disorder. The epidemic is the subject of numerous media publications, books and scientific articles, and public rallying cries. Numerous researchers and advocacy groups point to the “mental illness epidemic” as a major public health crisis. A 2017 WHO report even states that depression is the leading cause of disability worldwide. Drug companies, governments, nonprofits, and laypeople alike use claims of a “mental illness epidemic” in pushing for changes to mental health treatment (expanding care, developing new drugs, challenging stigma, etc.).
The anti-psychiatry movement goes further, blaming psychiatric treatments themselves for the crisis. Robert Whitaker argues that the rise of mental illness is due to the harmful effects of psychiatric drugs. He writes, “The percentage of Americans disabled by mental illness has increased fivefold since 1955, when Thorazine–remembered today as psychiatry’s first “wonder” drug–was introduced into the market” (Whitaker, 2005). In this paper, and in his book by the same name, Whitaker cites several studies as evidence of a stark rise in mental illness over the past few decades. This rise correlates with the landmark development and increased usage of psychiatric drugs (two major ones being Thorazine and Prozac).
There are two parts to this argument. The first is that rates of mental illness have drastically increased. Whitaker often cites a rise in mental illness-related disability claims (reported by the Social Security Administration) to demonstrate this. He finds that the number of people disabled by mental illness in the US increased by 149,739 every year since 1987, when Prozac was introduced.
The second part of the anti-psychiatry argument is that psychiatric drugs themselves contribute to the mental illness epidemic. Whitaker writes, “The drugs increase the likelihood that a person will become chronically ill, and induce new and more severe psychiatric symptoms in a significant percentage of patients” (Whitaker). Basically, patients’ brains adapt to the drugs, potentially leading to dependence/addiction or a higher tolerance (necessitating a higher dosage to maintain therapeutic effect). Because these drugs induce changes in brain chemistry, he argues that patients become more vulnerable to relapse after (or even during) treatment. Indeed, the studies he cites show worse outcomes for treatment groups vs. placebo groups over long periods of time–longer than the range of most Big Pharma-sponsored clinical trials. Furthermore, he finds a positive correlation between dosage size and chance of relapse.
The evidence Whitaker presents seems, at first glance, to be convincing proof of a mental health epidemic in the US. On the one hand, he demonstrates a rise in mental illness cases. On the other, he shows how treatment actually leads to a greater chance of relapse and long-term disability, thus contributing to the rise in cases of diagnosis/treatment. The book is well-respected among today’s anti-psychiatry movement and others who are skeptical of psychiatric drugs. I read it myself during my first week off of my medications. It helped me ground my decision in science, so I didn’t worry that my decision was just “treatment non-compliance” (a symptom of my diagnosed condition!).
However, upon review, I think the book has some issues. To be clear, I made the right decision for my health, and I’m grateful to this book for supporting me through that. But that certainly doesn’t mean the book is free from criticism. While I agree with certain points, some of the conclusions Whitaker draws are flawed and misleading. This is a problem I have with a lot of anti-psychiatry arguments, and the conversation around mental illness in general.

First of all, it’s hard to accurately assess rates of mental illness in a population. Many statistics on rates of mental illness rely on standardized surveys rather than structured clinical interviews. In “The epidemic in mental illness: clinical fact or survey artifact?” Horwitz and Wakefield write, “inflated rates stem from standard questions about symptoms with no context provided that might distinguish the normal distress experienced in life from genuinely pathological conditions that indicate an underlying mental illness” (Horwitz and Wakefield, 2006). Surveys lack the context necessary to rule out normal reactions to life events. These reactions are instead categorized as symptoms of illness, inflating results.
“The absence of interviewer probes can produce seriously misleading results. For example, when asked, “Have you ever had a period of two weeks or more when you had trouble sleeping,” a person might recall a time when ongoing construction across the street interrupted her sleep. In such a case, she can disregard the literal meaning of the question, self-censor her response, and not report the “symptom.” Or she can give an answer that is literally true, with the result that her troubled sleep will be counted as a potential symptom of a mental illness. The lack of clinical judgment based on exploring context can easily inflate reported rates of pathological conditions.” (Horwitz and Wakefield).
Because community surveys have this tendency to over-report, they’re probably not accurate measures for actual cases of mental illness. Instead, they contribute to a “pervasive medicalization of many problems that we might view more constructively as expectable results of social circumstances” (Ibid.). These surveys are not sufficient evidence for a increase in rates of actual mental illness (whatever that might mean).
Even the data from clinical interviews is problematic. It’s skewed by a strong self-selection bias–only those who seek treatment are recorded, leaving out anyone who would meet diagnostic criteria but don’t seek help. There are many reasons for this. Perhaps stigma, cultural differences, or alternate explanations for psychic distress discourage certain people from seeking help (from psy-professionals at least). Another very common issue is that some people just don’t have access to care, because it’s too expensive or it’s unavailable in their geographic region.
What about mental-illness related disability claims as a proxy metric for rates of mental illness? In a Psychiatric Times article, Ronald Pies writes, “it’s important to distinguish actual increases in illness frequency from the issues of alleged ‘over-diagnosis’ or ‘over-medication'” (Pies, 2015). There may be contributing factors to a disability determination beyond actual mental illness.
“Disability determinations by the Social Security Administration are largely administrative hearings–not medical-psychiatric evaluations–and are subject to a myriad of confounding variables. The outcome may depend, for example, on how well-prepared the applicant is when presenting his or her “case” to the evaluator–who may or may not have medical or psychiatric expertise.” (Pies).
Whitaker’s use of SSDI/SSI metrics entirely glosses over potentially confounding variables. Firstly, socioeconomic conditions changed drastically between 1955 and 2003. The rise of neoliberalism during this period resulted in welfare cuts and other policy changes, guided by a new paradigm of austerity. Perhaps disability has become a more viable option than other forms of welfare for those in need of assistance. Secondly, two new versions of the DSM emerged during this time period. Perhaps changes in diagnostic criteria have affected the prevalance of certain disability claims. Finally, the number from 1955 actually comes from a different source than the numbers for years following. Whitaker compares rates of hospitalization in 1955 to rates of SSDI/SSI payments in 1987 and 2003. I’m not at all convinced that these two metrics are commensurable. Nevertheless, they appear on the same chart.
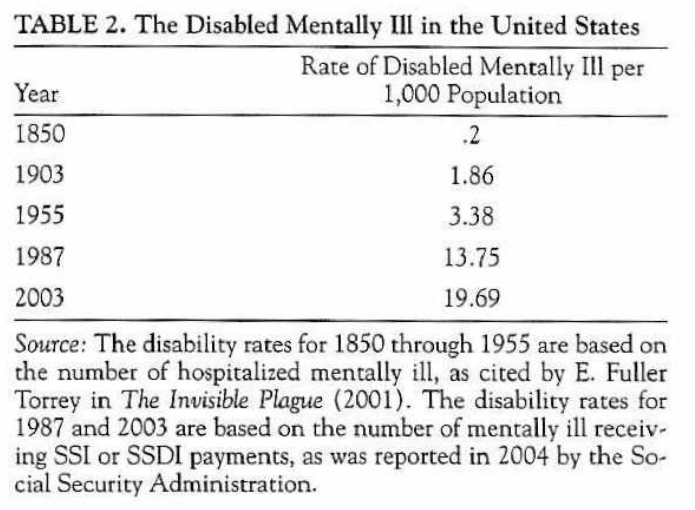
I also wonder about the rates of illness during the years not listed here. He lists the data for 1987 because this was the year Prozac was introduced. But is this the starting point of the upward trend in mental illness? What does the data look like for 1986 or 1985? We’re led to believe that 1987 marked the second surge in rates of mental illness (the first being in 1955 with Thorazine). But the only reason we’re led to believe this is because all the data in between is omitted. I’d have to look into study he cites here to find out if 1987 is markedly different from the years right before it. It seems like he selected this year because it fits his argument, and I’m left to wonder what information is conveniently left out.
This lack of data isn’t necessarily Whitaker’s fault. A big problem in psychiatric epidemiology is the lack of reliable data which tracks the same variables over long periods of time. Pies writes, “our methods for tracking the occurrence of psychiatric disease over long stretches of time are very limited.” Problems include self-selection bias in clinical settings, treatment availability, differing application of diagnostic criteria by individual doctors, new data collection methods, etc. The result is that it’s hard to find good proxy metrics for actual rates of mental illness in a population, especially over long periods of time.
Finally (we’ve all heard this one)… correlation is not causation! Even if rising disability claims or other metrics seem to correlate with the availability of prescription medications, they may both be results of some other underlying cause. Socioeconomic conditions, as mentioned above, bear considering. Many theorists (Mark Fisher, Byung-Chul Han) have argued that contemporary capitalism creates the conditions for psychic distress. Another factor to consider is the increasing psychologization of our society–the more we understand ourselves in psychological or psychiatric terms, the more likely we are to blame mental illness for our woes.
There are also many groups that benefit from a cultural belief in the “mental illness epidemic.” This isn’t limited to the obvious profit incentive for drug manufacturers. Horwitz and Wakefield write, “During the 1960s the National Institute of Mental Health (NIMH) promoted an expansive agenda of community mental health and sponsored projects that attempted to alleviate poverty, combat juvenile delinquency, and promote social change, but political changes in the 1970s forced the NIMH to change its focus from social and economic problems to specific diseases.” Spurred by a shift in politics, scientific treatment of illnesses became more legitimate (and worthy of continued funding) than efforts for social change. Over-reporting may also help advocacy groups by demonstrating how common mental illnesses are, reducing stigma towards the mentally ill.
There’s no conclusive proof of a “mental illness epidemic” in the US. Maybe it’s real, but it’s hard to say for sure. What’s definitely real is our belief in such a thing, and the effects of that belief. Whether or not rates of mental illness are increasing, there’s an active discourse around this topic, inside and outside of academia. This discourse affects how we think about ourselves and the world around us. It informs the decisions of both policymakers and everyday people navigating the ups and downs of life. Even if there’s no empirical evidence for a “mental illness epidemic,” the ongoing discussion of this concept is a worthy object of investigation.
Works Cited:
- Whitaker, Robert. “Anatomy of an epidemic: Psychiatric drugs and the astonishing rise of mental illness in America.” Ethical Human Psychology and Psychiatry 7.1 (2005): 23.
- Horwitz, Allan V., and Jerome C. Wakefield. “the epidemic in mental illness: clinical fact or survey artifact?.” Contexts 5.1 (2006): 19-23.
- Pies, Ronald. “The Bogus “Epidemic” of Mental Illness in the US.” Psychiatric Times. https://www.psychiatrictimes.com/view/bogus-epidemic-mental-illness-us